|
Một số bệnh phổi do nhiễm ký sinh trùng ở người (Phần 3-Hết)
Tiếp theo Phần 2
Bệnh giun chỉ phổi (Pulmonary dirofilariasis)
Bệnh ký sinh trùng này do giun chỉ Dirofilaria immitis gây ra. Muỗi truyền ký sinh trùng từ chó sang người. Bệnh giun chỉ được chẩn đoán nhiều nhất ở bờ biển phía đông và các vùng phía nam của Mỹ, với các trường hợp hiếm gặp ở những nơi khác trên thế giới. Một nghiên cứu gần đây từ Bán đảo Balkan đã báo cáo rằng hai trong số 46 trường hợp mắc giun chỉ bị nhiễm trùng phổi. Bệnh thường không có triệu chứng và biểu hiện dưới dạng một nốt phổi đơn độc cần phẫu thuật cắt bỏ. Bệnh không có hình ảnh X-quang hoặc triệu chứng cụ thể để phân biệt với các tổn thương phổi đơn độc khác. 
Hình. Tổn thương bệnh học ở phổi và phế nang do Dirofilaria immitis
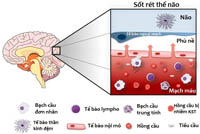
Biểu hiện ở phổi của bệnh sốt rét Sốt rét do ký sinh trùng Plasmodium falciparum, P. vivax, P. ovale và Plasmodiumspp. gây ra và lây truyền qua muỗi Anopheles. Các triệu chứng chính của bệnh sốt rét là sốt, ớn lạnh, đổ mồ hôi, thiếu máu các loại và lách to. Biểu hiện ở phổi thường gặp nhất của bệnh sốt rét là hội chứng suy hô hấp cấp tính và đây là một trong những tiêu chuẩn của bệnh sốt rét ác tính. Các biểu hiện khác ở phổi bao gồm tràn dịch màng phổi, sưng phù liên mô và đông đặc. 36% bệnh nhân nhiễm P. falciparum và 53% bệnh nhân nhiễm P. vivax hoặc P. ovale đã được mô tả là có triệu chứng ho thoáng qua. Ngoài ra, thông qua xét nghiệm khí quản, đã chỉ ra sự tắc nghẽn lưu thông khí cận lâm sàng cũng như xảy ra tình trạng trao đổi khí bị suy giảm. 
Hình. Thay đổi mô bệnh học ở phổi trong sốt rét ác tính P. falciparum
Ngoài ra, các biểu hiện khác bao gồm viêm phế quản tổ chức vô thể (bronchiolitis obliterans organising pneumonia: một loại viêm phổi mạn tính, trong đó mô tổ chức phủ kín các phế quản, gây ra các triệu chứng như ho, khò khè và khó thở do giảm sự thông khí). Chẩn đoán thường được thực hiện bằng cách xác định các thể tư dưỡng hoặc các thể ký sinh trùng khác trong hồng cầu ởlam máu mỏng hoặc ký sinh trùng ởlam máu dày. Các xét nghiệm kháng nguyên và xét nghiệm tăng sinh axit nucleic cũng có sẵn để hỗ trợ trong quá trình chẩn đoán. Điểm lưu ý trong thực hành lâm sàng |  Nhiều loại ký sinh trùng có thể gây ra bệnh phổi do quá trình di chuyển tạm thời qua phổi hoặc do phản ứng miễn dịch. Nhiều loại ký sinh trùng có thể gây ra bệnh phổi do quá trình di chuyển tạm thời qua phổi hoặc do phản ứng miễn dịch.
Biểu hiện lâm sàng của các bệnh phổi do ký sinh trùng có thể đa dạng, bao gồm các tổn thương khu trú hoặc dạng nang, tràn dịch màng phổi, hoặc các thâm nhiễm phổi lan tỏa. Các hội chứng đặc biệt quan tâm: hội chứng Loeffler, viêm phổi nhiệt đới (TES), và ấu trùng di chuyển nội tạng (VLM-visceral larva migrans). Với sự gia tăng toàn cầu hóa, các bệnh phổi do ký sinh trùng có thể xuất hiện ở những người đi du lịch hoặc di cư. |
Kết luận Sự liên quan đến phổi của các bệnh ký sinh khác nhau đã được biết đến rộng rãi trên toàn cầu. Các biểu hiện phổ biến nhất liên quan đến các bất thường trên X-quang, có thể xuất hiện các nốt đơn độc ở phổi. Các biểu hiện khác có thể phản ánh sự liên quan mang tính hệ thống và điều quan trọng là phải nhận biết những triệu chứng này để chẩn đoán và quản lý thích hợp, đặc biệt là đối với những người đi du lịch và nhóm dân di cư từ vùng không lưu hành đến vùng lưu hành bệnh.
Tài kiệu tham khảo
1.SantelizJV.Tropicalpulmonary eosinophilia:anepidemiologicalandclinicalreview.Int J RespirPulm Med2019;6:102. 2.KunstH,MackD,KonOM,etal.Parasiticinfectionsofthelung:aguidefortherespiratoryphysician.Thorax2011;66: 528-536. 3.Pérez-ArellanoJL,AndradeMA,López-AbánJ,etal.Helminthsandtherespiratorysystem.Arch Bronconeumol2006;42:81-91. 4.FujimuraJ,MurakamiY,TsudaA,etal.AneonatewithLöfflersyndrome.JPerinatol2001;21:207–208. 5.RibeiroJD,FischerGB.Eosinophiliclungdiseases.PaediatrRespirRev2002;3:278–284. 6.Shorman M, Al-Tawfiq JA. Strongyloides stercoralis hyperinfection presenting as acute respiratory failure and Gram-negative sepsis in a patient with astrocytoma. Int J InfectDis 2009; 13: e288–e291. 7.RajapurkarM,HegdeU,RokhadeM,etal.RespiratoryhyperinfectionwithStrongyloidesstercoralisina patientwithrenalfailure.NatClinPractNephrol2007;3:573-577. 8.Weingarten R J. Tropical eosinophilia. Lancet 1943; 1: 103–105. 9.Chitkara RK, Krishna G. Parasitic pulmonary eosinophilia. SeminRespirCritCareMed2006;27:171-184. 10.JoobB,WiwanitkitV.Filarialtropicalpulmonaryeosinophilia.JAsthma2020;57:230. 11.CanoJ,RebolloMP,GoldingN,etal.Theglobaldistributionandtransmissionlimitsoflymphaticfilariasis: pastandpresent.ParasitVectors2014;7:466. 12.Boggild AK, Keystone JS, Kain KC. Tropical pulmonary eosinophilia: a case series in a setting of nonendemicity. ClinInfectDis 2004; 39: 1123–1128. 13.LobosE,NutmanTB,HothersallJS,etal.ElevatedimmunoglobulinEagainstrecombinantBrugiamalayi γ-glutamyl transpeptidase in patients with bancroftian filariasis: Association with tropical pulmonary eosinophiliaorputativeimmunity.InfectImmun2003;71:747–753. 14.Sharma P, Sharma A, Ganga L, et al. Acidic calcium-independent phospholipase A2 regulates eosinophil-mediatedpathologyduringfilarialmanifestationoftropicalpulmonaryeosinophilia.JImmunol 2021;206:722–736. 15.Tsanglao WR, Nandan D, Chandelia S, et al. Filarial tropical pulmonary eosinophilia: a condition masqueradingasthma, a series of 12 cases. JAsthma2019; 56: 791-798. 16.Cooray JHL, Ismail MM. Re-examination of the diagnostic criteria of tropical pulmonaryeosinophilia. Respir Med1999;93:655-659. 17.NutmanTB,VijayanVK,PinkstonP,etal.Tropicalpulmonaryeosinophilia:analysisofantifilarialantibody localizedtothelung.JInfectDis1989;160:1042-1050. 18.AngirishB,JankhariaB,SanghaviP.TheroleofHRCTintropicalpulmonaryeosinophilia.EurJRadiol2020; 131: 109207. 19.MadanM,GuptaP,MittalR,etal.Tropicalpulmonaryeosinophilia:effectofadditionofcorticosteroidsafter failureofdiethylcarbamazinetherapy.AdvRespirMed2017;84:51–54. 20.Vijayan VK, Sankaran K, Venkatesan P, et al. Effect of diethylcarbamazine on the alveolitis of tropical eosinophilia.Respiration1991;58:255-259. 21.Sakai S, Shida Y, Takahashi N, etal.Pulmonary lesionsassociated with visceral larva migrans due to Ascaris suumor Toxocaracanis:imagingof six cases.AmJRoentgenol2006; 186:1697–1702. 22.ChitkaraRK,SarinasPSA.Dirofilaria,viscerallarvamigrans,andtropicalpulmonaryeosinophilia.Semin RespirInfect1997;12:138-148. 23.DemirciM,UnlüM,FidanF,etal.Eosinophilicpneumoniaduetotoxocariasis:anadultcasereport.Turkiye parazitolojiiDerg2012;36:258-259. 24.InoueK,InoueY,AraiT,et al. Chroniceosinophilicpneumoniaduetoviscerallarvamigrans.Intern Med 2002;41:478-482. 25.MatsumotoN,TsubouchiH,SetoguchiK,etal.Clinico-radiologiccharacteristicsofpulmonaryviscerallarva migranscausedby Ascarissuum. InternMed2021;60: 2899-2903. 26.OkadaF,OnoA,AndoY,etal.PulmonarycomputedtomographyfindingsofviscerallarvamigranscausedbyAscarissuum.JComputAssistTomogr2007;31:402–408. 27.Khalil HM, Azab ME, Safar EH, et al.Immunodiagnostics of visceral toxocariasis. JEgyptSocParasitol1989; 19: 381–393. 28.DzudieA, Dzekem BS, Ojji DB, etal.Pulmonary hypertension in low- andmiddle-incomecountries with focus on sub-Saharan Africa. CardiovascDiagnTher2020; 10: 316–324. 29.GobbiF,TamarozziF,BuonfrateD,etal.Newinsightsonacuteandchronicschistosomiasis:doweneeda redefinition?TrendsParasitol2020;36:660–667. 30.ColleyDG,BustinduyAL,SecorWE,etal.Humanschistosomiasis.Lancet2014;383:2253–2264. 31.HoulderEL,CostainAH,CookPC,etal.Schistosomesinthelung:immunobiologyandopportunity.Front Immunol2021;12:635513. 32.VadalaR,ShamsiI,DabralC,etal.Pleuralschistosomiasismasqueradingastubercularpyopneumothorax: world’sfirstcasereport.LungIndia2021;38:183–185. 33.CnopsL,HuyseT,ManiewskiU,etal.AcuteschistosomiasiswithaSchistosomamattheei×Schistosoma haematobiumhybridspeciesinaclusterof34travelersinfectedinSouthAfrica.ClinInfectDis2021;72: 1693–1698. 34.Posada-MartínezEL,Gonzalez-BarreraLG,LiblikK,et al. Schistosomiasis&Heart-Onbehalfoftheneglected tropical diseases and other infectious diseases affecting the heart(the NET-Heart Project) [Esquistossomoseeocoração–emnomedasdoençastropicaisnegligenciadaseoutrasdoençasinfecciosasqueafetamo coração(ProjetoNET-Heart)].ArqBrasCardiol2022; 118:885-893. 35.HoeperMM,HumbertM,SouzaR,etal.Aglobalviewofpulmonaryhypertension.LancetRespirMed2016;4: 306-322. 36.Maarman GJ, Shaw J, Allwood B. Pulmonary hypertension in majority countries: opportunities amidst challenges. CurrOpinPulmMed2020; 26: 373–383. 37.Rahaghi FN, Hilton JF, Corrêa RA, et al. Arterial vascular volume changes with haemodynamics in schistosomiasis-associated pulmonary arterial hypertension. Eur Respir J 2021; 57: 2003914. 38.MickaelCS,GrahamBB.Theroleoftype2inflammationinSchistosoma-inducedpulmonaryhypertension. FrontImmunol2019;10:27 39.DeClevaR,HermanP,PuglieseV,etal.Prevalenceofpulmonaryhypertensioninpatientswith hepatosplenicmansonicschistosomiasis: Prospectivestudy.Hepatogastroenterology2003;50:2028–2030. 40.Barbosa MM, Lamounier JA, Oliveira EC, etal.Pulmonary hypertension in schistosomiasis mansoni. TransR SocTropMedHyg1996;90:663-665. 41.LapaM,DiasB,JardimC,etal.Cardiopulmonarymanifestationsofhepatosplenicschistosomiasis.Circulation 2009;119:1518-1523. 42.Nunes MCP,GuimarãesMH,DiamantinoAC,etal.Cardiacmanifestationsofparasiticdiseases.Heart2017; 103: 651-658. 43.DengQ,HuB,ZhangY,etal.SuspectedmyocardialinjuryinpatientswithCOVID-19:evidencefromfront-line clinicalobservationinWuhan,China.IntJCardiol2020;311:116-121. 44.ButrousG.Pulmonaryvasculardiseasesassociatedwithinfectiousdisease: Schistosomiasisandhuman immunodeficiencyviruses.ClinChestMed2021;42:71-80. 45.KassaB,LeeMH,KumarR,etal.ExperimentalSchistosomajaponicum-inducedpulmonaryhypertension. PLoSNeglTropDis2022;16:e0010343. 46.SaadMAH,El-AnwarNet al.,Bevacizumabasapotentialanti-angiogenictherapyinschistosomiasis:a double-edged,butadjustableweapon.ParasiteImmunol2020;42:e12724. 47.Sibomana JP, Campeche A, Carvalho-Filho RJ, etal.Schistosomiasis pulmonaryarterial hypertension. Front Immunol2020;11:608883. 48.FerrariTCA,AlbrickerACL,GonçalvesIM,etal.Schistosome-associatedpulmonaryarterialhypertension:a reviewemphasizing pathogenesis. FrontCardiovascMed2021; 8: 724254 49.BameflehH,Al-HussainGO.Secondaryspontaneouspneumothoraxcausedbypulmonaryschistosomiasis. Cureus2021;13:e18709. 50.MortierC,AubryC,L’OllivierC,etal.Schistosomahaematobiuminfectionwithpulmonaryinvolvementina traveller returning from Congo: a case report and systematic review of literature on nodular pulmonary schistosomiasis.TravelMedInfectDis2021;44:102182. 51.CiminiA,RicciM,ChiaravallotiA,etal.Ararecaseofpulmonaryschistosomiasis:18F-fluorodeoxyglucose positronemissiontomography/computedtomographyfindings.IndianJNuclMed2020;35:336-338. 52.Nakamura-UchiyamaF,MukaeH,NawaY.Paragonimiasis:AJapaneseperspective.Clin Chest Med 2002;23: 409-420. 53.NagayasuE,YoshidaA,HombuA,etal.ParagonimiasisinJapan:atwelve-yearretrospectivecasereview (2001-2012).InternMed2015;54:176-186. 54.LiKK,JinGY, KwonKS. Whatfindingson chestCTscan delaydiagnosis ofpleuropulmonaryparagonimiasis? Tomography2022;8:1493–1502. 55.FuruyaS,FukuiS,MaekawaY,etal.ParagonimuswestermaniasacauseofLöeffler’ssyndrome.IDCases 2022;27: e01427. 56.Nakamura-UchiyamaF,HiromatsuK,IshiwataK,etal.ThecurrentstatusofparasiticdiseasesinJapan. InternMed2003;42:222-236. 57.YoshidaA,DoanhPN,MaruyamaH.Paragonimus andparagonimiasisinAsia:anupdate.Acta Trop 2019;199:105074. 58.PezzellaAT,YuHS,KimJE.Surgicalaspectsofpulmonaryparagonimiasis.CardiovascDis1981;8:187-194. 59.ShamsuzzamanSM,HashiguchiY.Thoracicamebiasis.ClinChestMed2002;23:479-492. 60.LichtensteinA,KondoAT,VisvesvaraGS,etal.Pulmonaryamoebiasispresentingassuperiorvenacava syndrome.Thorax2005;60:350-352. 61.Zakaria A, Al-Share B, Al Asad K. Primary pulmonary amebiasis complicated with multicystic empyema. Case RepPulmonol2016;2016:8709347. 62.Şimşek S, Akgül Özmen C. Unusual imaging characteristics of thoracic hydatid disease. Radiol Bras 2022; 55:128-133. 63.ParlakE,KergetF,DemirdalT,etal.Theepidemiology,clinicalmanifestations,radiology,microbiology, treatment,andprognosisofechinococcosis:resultsofNENEHATUNstudy.Vector BorneZoonoticDis 2021;21: 948-954. 64.Aydin Y, Ulas AB, Ince I, et al. Evaluation of albendazole efficiency and complications in patients with pulmonary hydatid cyst. Interact Cardiovasc Thorac Surg 2022; 34: 245-249. 65.GargMK,SharmaM,GulatiA,etal.Imaginginpulmonaryhydatidcysts.WorldJRadiol2016;8:581-587. 66.KantarciM,BayraktutanU,KarabulutN,etal.Alveolarechinococcosis:spectrumoffindingsat cross-sectional imaging. Radiographics 2012; 32: 2053-2070. 67.MartínezS,RestrepoCS,CarrilloJA,etal.Thoracicmanifestationsoftropicalparasiticinfections:apictorial review.Radiographics2005;25:135-155. 68.KuzucuA.Parasitic diseases of the respiratory tract. Curr Opin Pulm Med 2006; 12: 212-221. 69.AhmedSK,EssaRA,BapirDH.Uniportalvideo-assistedthoracoscopicsurgery(u-VATS)formanagementof pulmonaryhydatidcyst:asystematicreview.AnnMedSurg2022;75:103474. 70.ÜlküR,YilmazHG, onat S,etal.Surgical treatmentof pulmonary hydatidcysts: reportof 139 cases.IntSurg, 2006;91: 77–81. 71.NahmiasJ,GoldsmithR,SoibelmanM,etal.Three-to7-yearfollow-upafteralbendazoletreatmentof68 patients with cystic echinococcosis (hydatid disease). AnnTropMedParasitol1994; 88: 295 - 304. 72.UsluerO,KayaSO,SamancilarO,etal.Theeffectofpreoperativealbendazoletreatmentonthecuticular membranes of pulmonary hydatid cysts: Should it be administered preoperatively? Kardiochirurgia i TorakochirurgiaPol2014;11:26- 29. 73.Dehkordi AB, Sanei B, Yousefi M, etal.Albendazole and treatment of hydatid cyst, review of literature. Infect DisordDrugTargets2019;19:101- 104. 74.Arif SH, Shams-Ul-Bari, Wani NA, et al. Albendazole as an adjuvant to the standard surgical management of hydatidcystliver.IntJSurg2008;6:448 - 451. 75.KeramidasD,MavridisG,SoutisM,etal.Medicaltreatmentofpulmonaryhydatidosis:complicationsand surgical management. Pediatr Surg Int 2004; 19: 774 - 776. 76.Akhan O, Özmen MN, Dinçer A, et al. Percutaneous treatment of pulmonary hydatid cysts. Cardiovasc InterventRadiol1994; 17: 271-275. 77.GabalAM,KhawajaFI,MohammadGA.ModifiedPAIRtechniqueforpercutaneoustreatmentofhigh-risk hydatid cysts. CardiovascInterventRadiol2005; 28:200 - 208. 78.AsimacopoulosPJ,KatrasA,ChristieB.Pulmonarydirofilariasis:thelargestsingle-hospitalexperience.Chest, 1992;102:851–855. 79.SahaBK,BonnierA,ChongWH,etal.Humanpulmonarydirofilariasis:areviewfortheclinicians.AmJMed Sci2022;363:11-17. 80.MomčilovićS,GabrielliS,ĐenićN,etal.NewcasesofhumandirofilariosisontheBalkanPeninsula “Maskedintruders”uncoveredbyasurgeon.ParasitolInt2022;86:102482. 81.MiterpákováM,AntolováD,RampalováJ,etal.Dirofilariaimmitispulmonarydirofilariasis,Slovakia.Emerg InfectDis2022;28:482–485. 82.TakeiD,YamakiM,NoriyukiT,etal.Pulmonarydirofilariasis.KyobuGeka2015;68:76-79. 83.Al-Tawfiq JA.Epidemiologyoftravel-relatedmalaria in anon-malariousareas inSaudi Arabia.SaudiMedJ, 2006;27:1781-1782. 84.TaylorWRJ,WhiteNJ.Malariaandthelung.ClinChestMed2002;23:457-468. 85. TaylorWRJ,CañonV,WhiteNJ.Pulmonarymanifestationsofmalaria:Recognitionandmanagement.Treat RespirMed2006;5:419-428. 86.TaylorWRJ,HansonJ,TurnerGDH,etal.Respiratorymanifestationsofmalaria.Chest2012;142:492-505. 87.Anstey NM, Jacups SP, Cain T, etal.Pulmonary manifestations of uncomplicated falciparum and vivax malaria: cough, small airways obstruction, impaired gas transfer, and increased pulmonary phagocytic activity.JInfectDis2002;185:1326-1334. 88. YaleSH,AdlakhaA,SeboTJ,etal.BronchiolitisobliteransorganizingpneumoniacausedbyPlasmodium vivaxmalaria.Chest1993;104:1294-1296.
|